
 English
English German
German Spanish
Spanish Italian
Italian Japanese
Japanese United states
United states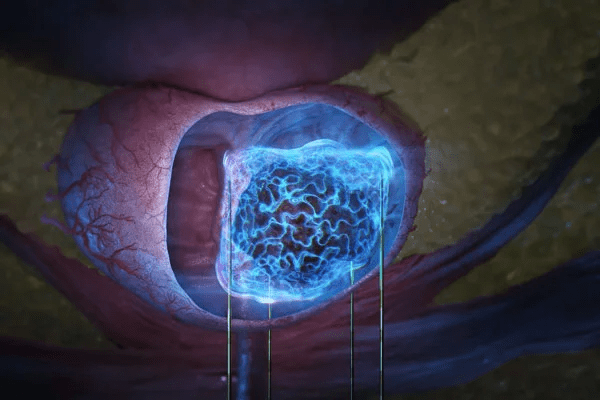
As technology advances and innovations in medicine evolve, new treatments for prostate cancer (PCa) emerge. Traditionally, newly diagnosed prostate cancer is treated with radical interventions such as prostatectomy or, conversely, monitoring with active surveillance. But minimally invasive treatment options, known as focal therapy, offer an alternative solution.
One of these solutions is irreversible electroporation (IRE), commercially known as the NanoKnife System. This innovative focal therapy treatment has demonstrated exceptional safety and favorable outcomes in both sexual and urinary function¹. Specifically, patients with localized clinically significant prostate cancer see the best outcomes with the NanoKnife System.
Continue reading to learn more about this innovative approach to prostate cancer treatment and how to get started with irreversible electroporation at your practice.
The Shift in Prostate Cancer Management

The continued shift in prostate cancer management is driven by enhanced diagnostic technology, particularly with advances in multiparametric magnetic resonance imaging (mpMRI) and fusion-guided prostate biopsy. These advances have resulted in the increased and precise identification of localized, intermediate-risk disease (Gleason Grade Group 2/3).
While standard treatments remain the benchmark for definitive oncologic control, they carry well-documented risks of treatment-induced morbidity and long-term urinary and sexual function side effects². This persistent trade-off between curative intent and quality of life necessitates the exploration of function-sparing alternatives for appropriately selected patients.
Ablation for Prostate Cancer
Ablation for prostate cancer is a strategic treatment approach aiming to eradicate malignant tissue while minimizing the destruction of surrounding healthy prostatic parenchyma. This concept is central to focal therapy, which seeks to treat only the known, clinically significant lesion(s).
Focal therapy modalities can be broadly categorized by their energy source. Techniques like High-Intensity Focused Ultrasound (HIFU), cryotherapy, and radiofrequency ablation (RFA) rely on thermal energy to induce coagulative necrosis. Irreversible electroporation, however, distinguishes itself as a uniquely non-thermal ablation technique. This differentiation at the cellular level is fundamental to IRE’s therapeutic advantages, particularly in the vicinity of critical structures.
The NanoKnife System

Commercially known as the NanoKnife System, IRE utilizes specialized electrodes and a high-voltage pulse generator to deliver controlled electrical fields directly to the target tissue. Using MRI-ultrasound fusion, surgeons have the ability to visualize the prostate and place electrodes with accuracy.
NanoKnife’s ability to achieve precise cell death while preserving the vital structures surrounding the prostate has positioned it as a highly promising modality within the focal therapy paradigm³. As we will discuss, clinical data from the PRESERVE Study (2025) validates the effectiveness of the NanoKnife System.
Patient Selection and Procedural Technique
Successful irreversible electroporation (IRE) outcomes are highly dependent on meticulous patient selection and precise procedural execution. Patients must have clinically localized disease, meaning the tumor is confined to the prostate and hasn’t spread to surrounding structures.
The primary target group for focal therapy are men with intermediate-risk prostate cancer, specifically Gleason Score 3+4 (ISUP Grade Group 2). Selected patients with very low-volume Gleason Score 4+3 (ISUP Grade Group 3) disease, where the lesion is small and anatomically favorable (e.g., anteriorly located), may also be candidates⁴.
Additionally, given that prostate cancer is often a slow-growing disease, candidates must have a reasonable chance to benefit from the treatment’s long-term outcomes, typically requiring a life expectancy of ten years or longer.
Pre-Procedural Workup and Targeting
Accurate targeting is the foundation of effective focal IRE, and mandatory use of mpMRI is essential for identifying and localizing the index lesion (the most significant tumor focus).
Confirmation of the malignant lesion is also mandatory. This is achieved through MRI-ultrasound fusion targeted biopsies of the index lesion. Crucially, a systematic biopsy of the remainder of the prostate is also performed to rule out out-of-field significant disease that would contraindicate a focal approach.
Clinical Outcomes and PRESERVE Study
The most comprehensive data point for focal IRE comes from the PRESERVE Study, which evaluated patients with intermediate-risk localized prostate cancer⁵.
The primary efficacy endpoint of the study was the negative in-field biopsy rate at 12 months. The trial’s clinically meaningful rate for patients who completed the follow-up biopsy was 84 percent (89/106). The rate for the entire intent-to-treat cohort, including those without a 12-month biopsy, was 71% (86/121). This data supports the device’s clearance and demonstrated effective short-term ablation within the targeted zone.
While IRE is widely studied, large-scale, randomized, long-term data (>5 years) is still limited compared to established standards like radical prostatectomy and External Beam Radiation (EBRT)⁶.
Final Thoughts
For men with intermediate-risk disease, IRE effectively controls the cancerous lesion while drastically minimizing the risk of severe side effects, such as permanent erectile dysfunction and urinary incontinence, thereby significantly prioritizing the patient’s quality of life.
However, IRE’s effectiveness is entirely dependent on the accurate placement of high-voltage electrode needles. With MRI-ultrasound fusion, surgeons can track the prostate and compensate for subtle patient movement and prostate deformation throughout the procedure.
Sources & References
1 – Faiella E, Santucci D, Vertulli D, Vergantino E, Vaccarino F, Perillo G, Beomonte Zobel B, Grasso RF. Irreversible Electroporation (IRE) for Prostate Cancer (PCa) Treatment: The State of the Art. J Pers Med. 2024 Jan 25;14(2):137. doi: 10.3390/jpm14020137. PMID: 38392571; PMCID: PMC10890194. https://pmc.ncbi.nlm.nih.gov/articles/PMC10890194/
2 – Stanford JL, Feng Z, Hamilton AS, Gilliland FD, Stephenson RA, Eley JW, Albertsen PC, Harlan LC, Potosky AL. Urinary and sexual function after radical prostatectomy for clinically localized prostate cancer: the Prostate Cancer Outcomes Study. JAMA. 2000 Jan 19;283(3):354-60. doi: 10.1001/jama.283.3.354. PMID: 10647798. https://pubmed.ncbi.nlm.nih.gov/10647798/
3 – Scheltema MJ, Geboers B, Blazevski A, Doan P, Katelaris A, Agrawal S, Barreto D, Shnier R, Delprado W, Thompson JE, Stricker PD. Median 5-year outcomes of primary focal irreversible electroporation for localised prostate cancer. BJU Int. 2023 Jun;131 Suppl 4:6-13. doi: 10.1111/bju.15946. Epub 2022 Dec 28. PMID: 36495481. https://pubmed.ncbi.nlm.nih.gov/36495481/
4 – Ghoreifi, A., Gomella, L., Hu, J.C. et al. Identifying the best candidate for focal therapy: a comprehensive review. Prostate Cancer Prostatic Dis 28, 684–692 (2025). https://doi.org/10.1038/s41391-024-00907-y
5 – PRESERVE Study | Clinical Studies & Research. AngioDynamics. https://www.angiodynamics.com/studies/preserve/
6 – Li R, Liu X, Yang B, Qiu J. External beam radiotherapy for prostate cancer: What are the current research trends and hotspots? Cancer Med. 2021 Jan;10(2):772-782. doi: 10.1002/cam4.3700. Epub 2021 Jan 21. PMID: 33480190; PMCID: PMC7877352. https://pmc.ncbi.nlm.nih.gov/articles/PMC7877352/