
 English
English German
German Spanish
Spanish Italian
Italian Japanese
Japanese United states
United states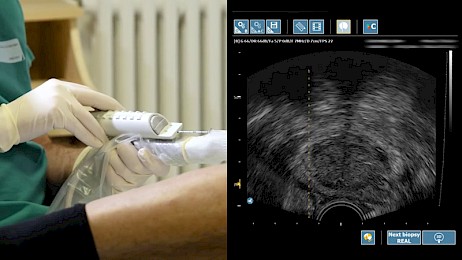
Whether you’re a physician, medical student, or patient facing the prospect of a prostate cancer diagnosis, conventional wisdom says that a transrectal prostate biopsy is the easiest and most cost-effective option for diagnosing cancer.
The transrectal (TR) prostate biopsy can be performed in a clinical setting, which means you often won’t need to check into a hospital and undergo general anesthesia for the procedure. Additionally, transrectal prostate biopsies don’t require advanced imaging technology, making them much more accessible and affordable for patients.
However, the transperineal (TP) prostate biopsy is becoming more popular for a variety of reasons. The advanced technology of transperineal fusion platforms have higher cancer detection rates and lower infection rates than transrectal biopsies¹.
Let’s dive deeper into the pros and cons of transperineal vs. transrectal prostate biopsy to understand the best option for both patients and medical professionals in the evolving field of prostate cancer.
“Studies show the advanced technology of transperineal fusion platforms have a higher cancer detection rate and lower infection rates than transrectal biopsies⁴. ”
The Transrectal Biopsy
Pictured above: The KOELIS transrectal probe and needle guide used in transrectal prostate biopsies.
A transrectal prostate biopsy is one of two main methods used by urologists to detect the presence of cancer in the prostate. This procedure is performed by inserting a needle through the rectum which allows for direct access to the prostate. Urologists performing a TR biopsy often use ultrasound imaging technology to visualize and target specific regions of the prostate.
Urologists collect 10-15 samples from the prostate during the biopsy that are sent to pathology to test for the presence of cancer. Pathology will also determine the grade and aggressiveness of the cancer so the doctor and patient have accurate information to make an informed decision for a treatment plan.
Pros of Transrectal Biopsy
While the transrectal biopsy is losing steam as the gold standard method to biopsy, there are still reasons why physicians are reluctant to switch to transperineal.
As we mentioned, transrectal biopsies are widely available across many healthcare settings and have been practiced by doctors since the introduction of transrectal ultrasound (TRUS) in the 1980s². This ultrasound technology makes it easy for doctors to quickly locate the prostate and obtain targeted samples for cancer detection.
Another major consideration for patients facing a prostate cancer diagnosis is the cost of biopsy procedures. As we’ll discuss later, the transperineal approach is often more sophisticated and uses MRI-ultrasound technology that may be too costly for some patients.
Additionally, transrectal biopsies are available in outpatient or office settings and may not require hospital admission. The procedure is only 10-15 minutes long and local anesthesia is used to numb the rectal area prior to the biopsy. This makes the TR biopsy a convenient option for patients who prefer a quick procedure without a hospital stay.
Cons of Transrectal Approach
As we mentioned, the transrectal (TR) prostate biopsy has long been the standard method for sampling prostate tissue. While this approach is widely practiced and familiar to many urologists, it carries several important drawbacks that have led to a growing preference for the transperineal (TP) route in recent years.
Infection Risk
One of the most significant concerns with TR biopsy is the risk of infection. Because the needle passes directly through the rectal lining, there is a higher likelihood of introducing bacteria into the prostate and bloodstream.
Despite the use of prophylactic antibiotics, post-biopsy infections and even sepsis remain a serious concern, with reported complication rates as high as 5 to 7 percent³.
Additional Complications
TR biopsies also come with a range of bleeding complications. Hematuria (blood in the urine) is common and typically resolves on its own, but rectal bleeding and hematospermia (blood in the semen) are also potential complications. Although usually limited, these side effects contribute to patient discomfort and anxiety during recovery.
Limited Targeting Ability
Another key limitation of the transrectal approach is its restricted access to certain regions of the prostate, particularly the anterior zone. These areas are more difficult to reach through the rectal wall and may result in missed clinically significant lesions.
For this reason, the transperineal approach is often preferred over the transrectal approach for enhanced targeting and patient comfort. With advanced MRI-ultrasound fusion systems, physicians can visualize the prostate gland with elastic fusion technology that seamlessly fuses the ultrasound and MR image sets together for a live 3D image of the prostate gland, leading to higher accuracy and increased confidence in treatment planning.
The Transperineal Biopsy
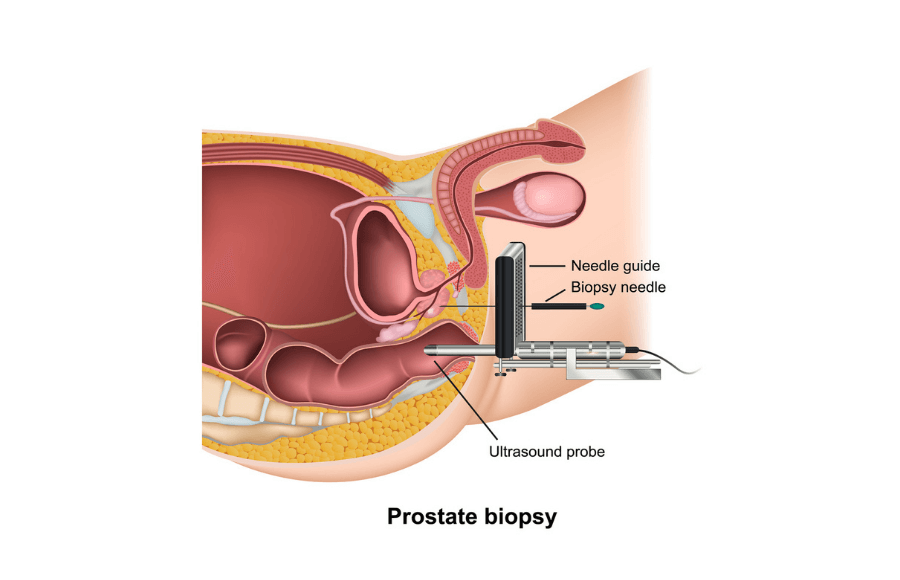
Above: Example diagram of a transperineal prostate biopsy.
Now that you understand the transrectal biopsy, its benefits, and why it’s not the most effective option when screening for prostate cancer, let’s talk about the transperineal biopsy and why more physicians are adopting this innovative approach.
Transperineal vs Transrectal Prostate Biopsy
Unlike the transrectal biopsy, a transperineal (TP) prostate biopsy is a method of obtaining prostate tissue samples by inserting biopsy needles through the perineum (the area between the scrotum and the anus) rather than through the rectum. Typically performed under local or general anesthesia, the TP biopsy can be done using a grid-based template or freehand.
This approach has gained significant momentum in recent years due to its enhanced safety profile and diagnostic capabilities, particularly in the era of precision medicine and MRI-visible lesion targeting.
3 Benefits of Transperineal Biopsy
Since the needle does not pass through the rectal wall, TP biopsy avoids direct contact with fecal bacteria. As a result, the risk of post-biopsy infection or sepsis is extremely low. In most cases, no antibiotics are needed, which also helps combat the rise of antibiotic resistance.
Higher Reimbursement
Hospitals and ambulatory surgery centers (ASCs) benefit with higher reimbursement when performing transperineal biopsies. The reason for higher reimbursement is due to transperineal biopsies using advanced technology compared to the transrectal approach that provides a higher standard of care.
Physicians and practices will see a higher return on investment (ROI) when adopting the transperineal approach, which allows them to increase biopsy volume and recoup their initial investment quickly while providing the highest quality care to patients.
Access to the Entire Prostate
The transperineal route provides improved access to the anterior and transition zones of the prostate, which are often under-sampled or missed entirely with the TR approach. This makes TP biopsy more effective for targeting MRI-visible lesions and reduces false negatives.
Additionally, physicians benefit from a more efficient workflow with the transperineal approach. Treatment planning and preparation is streamlined and physicians benefit from 3D cartography maps that aid in repeat biopsy and focal therapy planning.
Compatible with Local Anesthesia and Outpatient Settings
While earlier TP techniques often required general anesthesia, modern protocols using local anesthesia and precision needle guides have made it feasible to perform TP biopsies in an office-based setting. This reduces cost, streamlines workflow, and expands access to safer biopsy techniques.

3 Cons of Transperineal Prostate Biopsy
Most transperineal biopsy systems are expensive and will not be ideal for all physicians performing biopsies. Additionally, capital equipment purchases for prostate cancer biopsy systems often go through a rigorous and lengthy approval process in hospital environments and may not be approved after financial scrutiny.
Physician and Staff Onboarding
MRI fusion platforms present physicians and staff with an entirely new workflow that must be learned before biopsy procedures begin. This change in workflow can be stressful and lead to pushback from staff.
However, training and onboarding doesn’t have to be a grueling process. Fusion biopsy companies often have a dedicated clinical support team to provide training and onboarding before, during, and after first biopsy cases start.
Potential for Temporary Discomfort
Because the needles are inserted through the perineum, some patients may experience soreness, bruising, or swelling in the area afterward. Others may report urinary urgency or retention, though these are generally mild and self-limited.
“The transperineal route provides improved access to the anterior and transition zones of the prostate, which are often under-sampled or missed entirely with the TR approach.”
Final Thoughts
Whether you’re a patient, physcian, or hospital administrator, knowing the differences between transperineal vs. transrectal prostate biopsy is the first step in deciding the best method of biopsy for your practice.
Both transperineal and transrectal approaches offer unique benefits, but physicians looking to provide the highest standard of care are migrating to transperineal fusion biopsy systems for the TP approach. The advanced targeting, elastic fusion technology, and 3D cartography are just a few of the reasons why transperineal biopsy continues to emerge as a trusted biopsy method.
Ask your urologist about KOELIS, or find a certified provider in our network with our KOELIS Locator.
Sources & References:
1. Boesen L, Nørgaard N, et al. Office-based Magnetic Resonance Imaging-guided Transperineal Prostate Biopsy Without Antibiotic Prophylaxis: A Real-world Clinical Utility Study. Eur Urol Open Sci. 2023 Dec 23;59:71-77. doi: 10.1016/j.euros.2023.12.002. PMID: 38298768; PMCID: PMC10829603. https://pubmed.ncbi.nlm.nih.gov/38298768/
2. Schmeusser B, Levin B, Lama D, Sidana A. Hundred years of transperineal prostate biopsy. Ther Adv Urol. 2022 May 21;14:17562872221100590. doi: 10.1177/17562872221100590. PMID: 35620643; PMCID: PMC9128053.
3. Risk Factors for Infection after Prostate Biopsy in the United States. Shoag, Jonathan E. et al. Urology, Volume 138, 113 – 118
4. Cornud F, Roumiguié M, et al. Precision Matters in MR Imaging-targeted Prostate Biopsies: Evidence from a Prospective Study of Cognitive and Elastic Fusion Registration Transrectal Biopsies. Radiology. 2018 May;287(2):534-542. doi: 10.1148/radiol.2017162916. Epub 2018 Jan 22. PMID: 29361246. https://pubmed.ncbi.nlm.nih.gov/29361246/