
 English
English German
German Spanish
Spanish Italian
Italian Japanese
Japanese United states
United states
Prostate cancer is one of the most common types of cancer affecting men in the world today. Luckily, with innovations in technology and cancer detection, treating prostate cancer has never been more effective.
One of the most significant innovations in prostate cancer detection is the MRI fusion prostate biopsy. This method of detecting cancerous tissue in the prostate uses magnetic resonance imaging (MRI) data fused with a live ultrasound image to provide physicians with a highly accurate visualization of the prostate gland for better lesion targeting during biopsy.
While the MRI fusion prostate biopsy is still in the process of mass adoption by urologists, clinical evidence supports MRI-targeted biopsy approaches in many settings, and adoption has increased as more practices integrate prostate MRI into diagnostic pathways.
Let’s learn more about the MRI fusion prostate biopsy along with its benefits, drawbacks, procedure process, and clinical evidence that support this approach as the new gold standard for prostate biopsy.
“Physicians who aim to provide the best clinical outcomes for patients are migrating to MRI fusion.”
Types of Prostate Biopsy
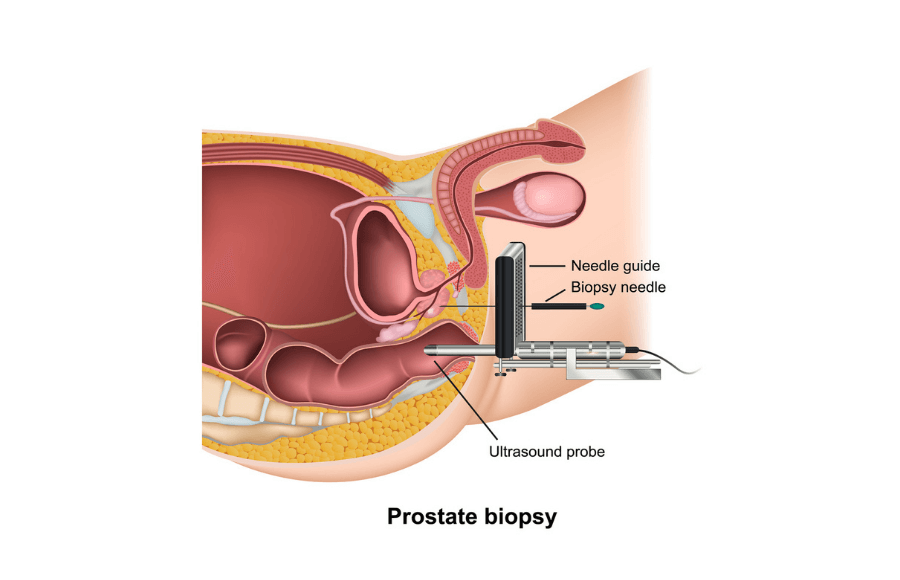
Above: Example diagram of a transperineal prostate biopsy.
Before we discuss the MRI fusion prostate biopsy specifically, it’s important to understand other common types of prostate biopsy that exist today.
Transrectal Ultrasound-Guided Biopsy (TRUS)
TRUS biopsy has been widely used for decades because it is accessible and office-based. However, systematic sampling can miss some clinically significant cancers, which is one reason MRI-targeted approaches have gained attention.
The TRUS biopsy uses ultrasound imaging via an ultrasound probe inserted into the rectum. The physician uses a biopsy needle to pierce the rectal lining and takes 10-12 core prostate samples, often without direct targeting of suspicious lesions.
The TRUS biopsy is known to cause patient discomfort and has a higher risk of infection. In fact, one study found that TRUS biopsy can be associated with side effects such as hematuria, hematospermia, urinary symptoms, and, in some cases, infection.¹. Additionally, the study found that patients are likely to have persistent hematuria for up to 3 to 7 days after the procedure.
“One study found among 128 TRUS biopsy patients, there were 135 minor complications. Additionally, 63 percent of patients had at least one complication after biopsy¹.”
Transperineal Ultrasound-Guided Biopsy (TPUS)
The transperineal ultrasound-guided biopsy (TPUS) is similar to the TRUS biopsy, as the procedure also uses ultrasound technology but accesses the prostate through the perineum. Since the biopsy needle doesn’t pass through the rectal lining, the risk of infection is lower with the TPUS approach.
However, without MRI targeting, transperineal biopsy may still rely on systematic sampling that can miss some lesions depending on tumor location and sampling strategy.
In-Bore MRI Biopsy
The in-bore MRI biopsy uses real-time MR images to guide the biopsy needle to specific areas of the prostate for tissue sampling. This method requires the patient to remain inside the MRI scanner during the procedure, and the T2-weighted images visualize both the suspicious lesion and the biopsy needle to confirm exact placement.
The in-bore MRI biopsy offers better accuracy and precision compared to TRUS and TPUS biopsies, but it’s a time-consuming and expensive procedure that has limited practicality for routine use.
What is an MRI Fusion Prostate Biopsy?
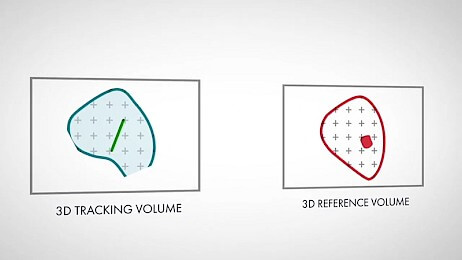
Above: Illustration of the live ultrasound tracking volume and pre-biopsy MRI reference volume before fusion.
Now that you understand other popular biopsy methods, let’s dive into the MRI fusion prostate biopsy to learn more about its effectiveness and why many practices are adopting MRI–ultrasound fusion approaches for targeted biopsy.
An MRI fusion prostate biopsy is a diagnostic procedure that combines multiparametric MRI (mpMRI) images of the prostate with real-time ultrasound imaging during the biopsy. The goal is to help target MRI-suspicious lesions during biopsy, which may improve detection of clinically significant cancer in appropriate patients.
In MRI–ultrasound fusion biopsy, MRI images with marked regions of interest are fused with real-time ultrasound to help guide targeted sampling. This allows physicians to now see the MRI-identified lesions within the live ultrasound view for enhanced targeting.
Similar to the TRUS and TPUS biopsy, the physician takes 10-12 samples of the prostate guided by the fused imaging. After each sample, many fusion platforms can record and display core locations to support documentation of sampling.
Benefits of MRI Fusion
As you’ll see, there are plenty of reasons why the MRI fusion is being adopted by leading medical institutions. Here are just a few:
Targeted Sampling of MRI-Suspicious Lesions
MRI–ultrasound fusion biopsy is designed to improve targeting of MRI-identified lesions. In fact, a 2018 study reported higher targeting precision with deformable MRI/ultrasound fusion compared with cognitive targeting in that study setting².
Another study in the New England Journal of Medicine (NEJM) found that an MRI pathway with targeted biopsy was associated with improved detection of clinically significant cancer and reduced detection of clinically insignificant cancer³.
Reduced Chances of Missed Cancer
Due to its accuracy in lesion targeting, using MRI fusion prostate biopsy system may reduce the chance of missing some cancers, especially lesions in locations that can be undersampled with systematic biopsy.
Flexible Approach
While some biopsy methods are rigid in their approach, the MRI fusion biopsy has flexibility to be performed either transperineally or transrectally depending on practice preference, patient factors, and local protocol.
“Due to its higher accuracy in lesion targeting, using MRI fusion prostate biopsy systems like KOELIS Trinity® results in fewer missed cancers.”
Drawbacks of MRI Fusion Prostate Biopsy
While the MRI fusion prostate biopsy is quickly gaining traction, there are some important drawbacks to consider before going all-in on this innovative technology.
Cost & Accessibility
The MRI fusion prostate biopsy requires advanced software and specialized biopsy platforms that some smaller clinics or urologists may not be able to afford. This drawback limits availability to patients outside of major hospitals and academic centers.
Technical Complexity
Using an MRI fusion biopsy system not only requires the urologist to become an expert with the system, but also requires hospital staff to become familiar with fusion software and a new biopsy system. The transition from an older system and the learning curve of the new platform can be a challenge.
MRI Fusion Prostate Biopsy Procedure

The patient is positioned in either the lithotomy or left lateral decubitus position depending on whether a transrectal or transperineal approach is used. The area is prepped and draped using standard sterile technique.
Multiparametric MRI data from a prior diagnostic exam are loaded into the fusion platform. Regions of interest (ROIs) identified on MRI are fused with the real-time ultrasound scan using KOELIS’ proprietary Organ-Based Tracking® (OBT) technology. Once fusion is confirmed, the physician selects target lesions from the MRI overlay and defines the number and location of cores to be extracted. Many fusion platforms provide 3D visualization and documentation of core locations within a prostate model.
The biopsy needle is aligned with the probe guide (transrectal) or introduced through the perineal grid or freehand (transperineal). The KOELIS system tracks the needle path and updates the 3D model dynamically while recording the spatial position of each core.
Once all planned cores have been obtained, the probe is withdrawn, the area is cleaned, and the patient is monitored briefly for any immediate complications. The KOELIS biopsy map is saved for use in longitudinal care such as follow-up biopsies, active surveillance, or focal therapy planning.
The Bottom Line
MRI-targeted biopsy has become more widely adopted and is supported by growing clinical evidence. The best approach depends on patient risk factors, imaging findings, and local expertise. MRI-targeted biopsy aims to improve lesion targeting and may help increase detection of clinically significant cancer.
Click here to learn more about KOELIS.
References
1 – Rodríguez LV, Terris MK. Risks and complications of transrectal ultrasound guided prostate needle biopsy: a prospective study and review of the literature. J Urol. 1998 Dec;160(6 Pt 1):2115-20. doi: 10.1097/00005392-199812010-00045. PMID: 9817335.
2 – Cornud F, Roumiguié M, Barry de Longchamps N, Ploussard G, Bruguière E, Portalez D, Malavaud B. Precision Matters in MR Imaging-targeted Prostate Biopsies: Evidence from a Prospective Study of Cognitive and Elastic Fusion Registration Transrectal Biopsies. Radiology. 2018 May;287(2):534-542. doi: 10.1148/radiol.2017162916. Epub 2018 Jan 22. PMID: 29361246.
3 – MRI-Targeted or Standard Biopsy for Prostate-Cancer Diagnosis. Veeru Kasivisvanathan, Antti S. Rannikko, Marcelo Borghi, et al. The New England Journal of Medicine. Massachusetts Medical Society. May 10, 2018.Copyright © 2018, Massachusetts Medical Society. https://www.nejm.org/doi/full/10.1056/NEJMoa1801993