
 English
English German
German Spanish
Spanish Italian
Italian Japanese
Japanese United states
United states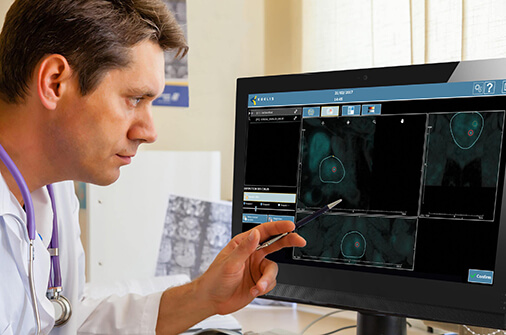
The field of prostate cancer detection has been fundamentally reshaped by the drive to distinguish between aggressive, life-threatening disease and indolent, low-grade cancer that may never cause harm. Historically, widespread PSA screening and systematic biopsies led to a significant problem of overdiagnosis and subsequent overtreatment¹.
Today, the clinical imperative is to focus squarely on identifying clinically significant prostate cancer (CS PCa). This pivot is not only critical for preventing overtreatment but also enables the rise of newer, preservation-focused options like irreversible electroporation (IRE), HIFU, and more.
This essential need for diagnostic accuracy has been powered by key technological advances, particularly the synergy between multiparametric MRI and targeted sampling. Consequently, the MRI-ultrasound fusion biopsy has rapidly emerged as the gold standard for precision. This approach provides the exact geographic coordinates needed to target suspicious lesions and ensure the most informed management decision.
Continue reading to learn more about clinically significant prostate cancer detection, its limitations, and clinical outcomes for patients with prostate cancer.
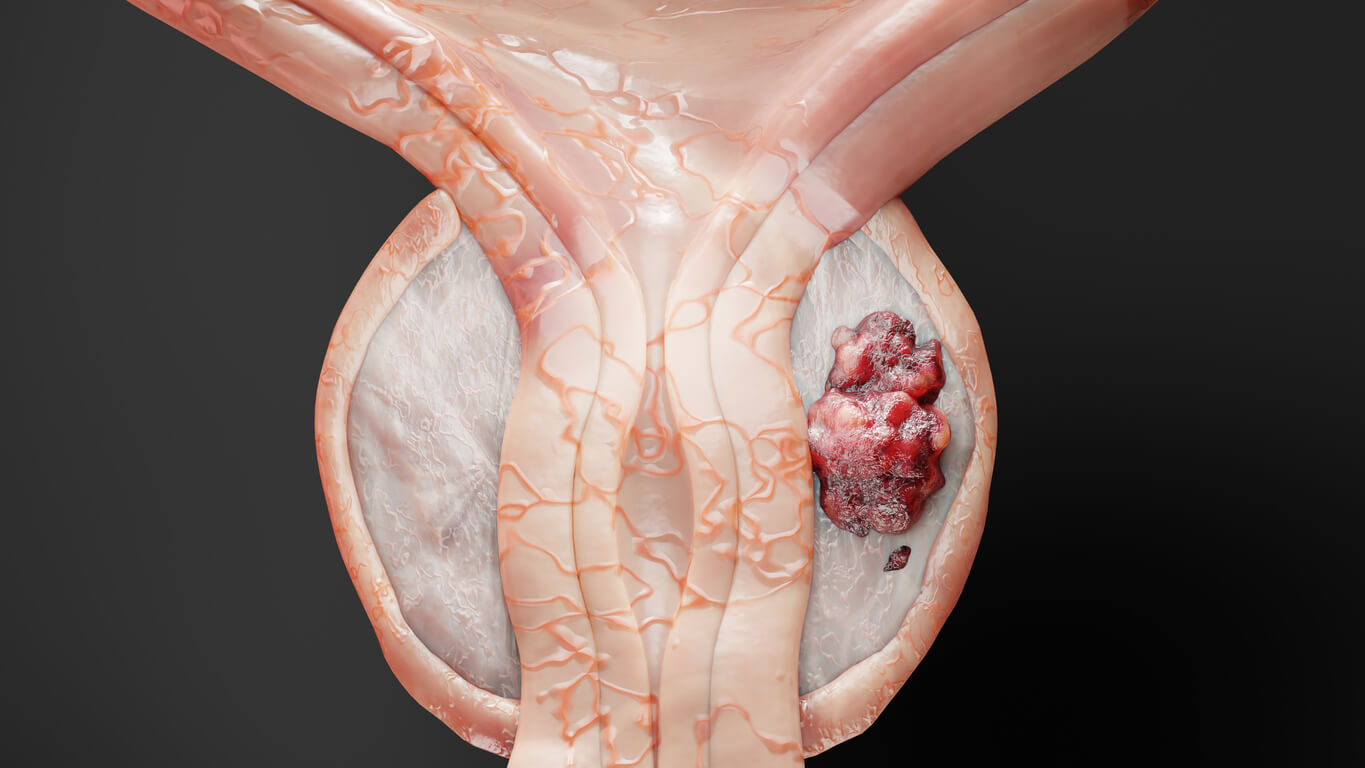
What is Clinically Significant Prostate Cancer?
While there is ongoing debate on what constitutes clinically significant prostate cancer², this concept provides an essential filter that allows clinicians to differentiate between tumors that require immediate intervention and indolent disease best managed by surveillance. CS PCa is primarily defined by its histological grade, which correlates directly with metastatic potential. The foundation of this definition relies on the Gleason grading system:
• Indolent/Low-Risk Disease: Gleason Score 6 (Grade Group 1). These tumors possess favorable biological behavior and are overwhelmingly managed via active surveillance.
• Clinically Significant Disease: Gleason Score 3+4=7 (Grade Group 2) or higher (GG 3, 4, 5).
• Grade Group 2 (3+4=7): Represents the lowest threshold for CS PCa. While some cases may qualify for active surveillance under stringent protocols, the presence of a tertiary grade 4 component signifies higher risk and often prompts curative intervention.
• Grade Group 3 (4+3=7) and above: These carry progressively higher risks of progression and metastatic spread, mandating definitive treatment (radical prostatectomy, radiation, or high-intensity focal therapy).
While grade is the dominant factor, tumor volume and extent are secondary characteristics contributing to significance. The general consensus dictates that clinically significant prostate cancer also includes tumor volume (typically defined as a lesion greater than 0.5 cm in maximal diameter) and stage of disease.
Limitations of Traditional Prostate Cancer Detection
Initial detection begins with the Prostate-Specific Antigen (PSA) blood test and the Digital Rectal Exam (DRE)³. Both serve an indispensable role as gatekeepers for further investigation, yet both are inherently limited in their ability to classify risk.
While PSA exhibits high sensitivity in detecting prostatic irregularities, its low specificity presents a major diagnostic challenge. Elevated PSA levels are not exclusive indicators of high-grade malignancy, as they can result from benign prostatic hyperplasia (BPH), prostatitis, or even recent prostatic manipulation.
The Era of Systematic Biopsy
Prior to the widespread adoption of MRI-based diagnostics, the gold standard for tissue acquisition was the transrectal ultrasound (TRUS)-guided systematic biopsy.
This procedure involved obtaining 10 to 12 standardized, predetermined cores from across the prostate gland while relying solely on real-time TRUS imaging. However, the principal failing of the systematic approach is the geographical miss⁴. When a biopsy is performed randomly, there is a significant risk of missing the high-grade tumor entirely, leading to a false-negative diagnosis.
Conversely, the systematic, wide-ranging sampling technique frequently led to the detection of minute, low-volume Gleason Score 6 (Grade Group 1) tumors. This overdetection of indolent disease was the direct cause of the overtreatment crisis, leading to the avoidable disadvantages associated with radical therapies⁵.
Detecting Clinically Significant Prostate Cancer

Above: Prostate biopsy map on KOELIS Trinity® showing biopsy targets.
The integration of advanced imaging with real-time biopsy guidance addresses the shortcomings of TRUS-guided systematic sampling, establishing the MRI-ultrasound fusion biopsy as the new gold standard for precision diagnostics. This technology specifically aims to confirm or rule out the presence of clinically significant prostate cancer by accurately sampling suspicious areas.
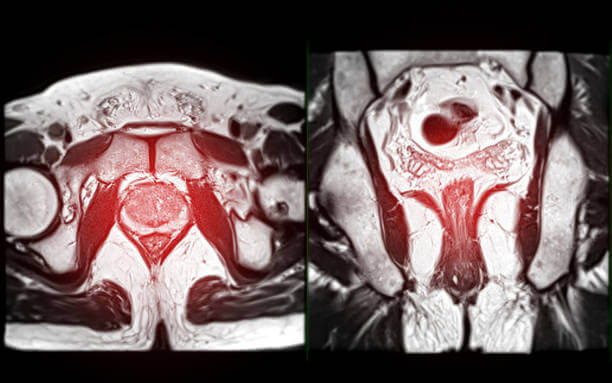
The foundation of the MRI-US fusion approach lies in harnessing the soft-tissue contrast of multiparametric magnetic resonance imaging (mpMRI), which is highly sensitive for clinically significant prostate cancer, and integrating this data with the real-time procedural advantages of transrectal or transperineal ultrasound.
Prior to the procedure, high-resolution mpMRI scans, annotated by a radiologist using the PI-RADS scoring standard, are loaded into the fusion platform. During the procedure, the fusion system overlays the pre-acquired three-dimensional MRI volume onto the two-dimensional, real-time ultrasound images. This provides the urologist with a persistent, virtual ‘map’ of the suspicious target.
A key technical necessity for successful fusion is compensating for patient movement and deformation of the prostate. When the probe is inserted and the gland is compressed for the ultrasound examination, its shape changes relative to the pre-biopsy MRI. Advanced systems like KOELIS Trinity® utilize elastic fusion to dynamically adjust the MRI map in real-time.
Treatment and Clinical Outcomes

The integration of mpMRI and elastic fusion technology fundamentally changes the diagnostic pathway, moving the focus from generalized screening toward individualized, risk-based patient management. The most compelling evidence supporting MRI-US fusion biopsy is its ability to overcome the ‘geographical miss’ and overdetection problems inherent to systematic sampling for higher precision than traditional techniques⁶.
For the large cohort of men found to have low-volume, low-grade cancer, weighing the pros and cons of radical treatment is necessary⁷. A negative MRI followed by a negative targeted biopsy, or a biopsy that only confirms Grade Group 1 disease, provides the highest level of confidence required for enrollment in active surveillance programs.
When clinically significant prostate cancer is confirmed, the fusion system’s data becomes indispensable for definitive treatment planning. The precise 3D localization of the tumor relative to critical structures, such as the neurovascular bundles (NVBs) responsible for erectile function, allows surgeons to perform highly targeted nerve-sparing radical prostatectomy.
For unifocal CS PCa, the precise, documented location and size of the tumor is the prerequisite for planning focal therapies (e.g., HIFU, cryotherapy). These ablative techniques aim to treat only the index lesion while preserving the majority of the prostate gland, thereby minimizing the risk of urinary and sexual side effects associated with whole-gland treatment⁸.
Final Thoughts
Clinically significant prostate cancer detection has increased in recent years with advancements in screening methods. With MRI-ultrasound fusion systems, physicians have an enhanced visualization of the prostate during biopsy with the added benefit of focal therapy planning features.
Looking to learn more about KOELIS Trinity 3D MRI-US fusion biopsy system? Contact us to discover the most advanced fusion platform trusted by top cancer institutions worldwide.
Sources & References
1 – Andrew B. Rosenkrantz, Samir S. Taneja. Prostate MRI Can Reduce Overdiagnosis and Overtreatment of Prostate Cancer. Academic Radiology. Volume 22, Issue 8, 2015. Pages 1000-1006. ISSN 1076-6332. https://doi.org/10.1016/j.acra.2015.02.006.
2 – Carlsson SV, Carroll PR, Hamdy FC. Reevaluating the Definition of Clinically Significant Prostate Cancer as Grade Groups 2 to 5: An Imperative for Improved Risk Stratification. Journal of Urology [Internet]. 2025 Feb 1 [cited 2025 Nov 3];213(2):238–41. Available from: https://doi.org/10.1097/JU.0000000000004253
3 – Carter HB, Partin AW, Walsh PC, Trock BJ, Veltri RW, Nelson WG, Coffey DS, Singer EA, Epstein JI. Gleason score 6 adenocarcinoma: should it be labeled as cancer? J Clin Oncol. 2012 Dec 10;30(35):4294-6. doi: 10.1200/JCO.2012.44.0586. Epub 2012 Oct 1. PMID: 23032616; PMCID: PMC3515766. https://pmc.ncbi.nlm.nih.gov/articles/PMC3515766/
4 – The Problem with Systematic Prostate Biopsy. HALO Precision Diagnostics. HALODx. August 25, 2020. https://www.halodx.com/blog/the-problem-with-prostate-biopsy/
5 – Bangma CH, Roemeling S, Schröder FH. Overdiagnosis and overtreatment of early detected prostate cancer. World J Urol. 2007 Mar;25(1):3-9. doi: 10.1007/s00345-007-0145-z. Epub 2007 Feb 14. PMID: 17364211; PMCID: PMC1913182. https://pmc.ncbi.nlm.nih.gov/articles/PMC1913182/
6 – Cornud F, Roumiguié M, Barry de Longchamps N, Ploussard G, Bruguière E, Portalez D, Malavaud B. Precision Matters in MR Imaging-targeted Prostate Biopsies: Evidence from a Prospective Study of Cognitive and Elastic Fusion Registration Transrectal Biopsies. Radiology. 2018 May;287(2):534-542. doi: 10.1148/radiol.2017162916. Epub 2018 Jan 22. PMID: 29361246. https://pubmed.ncbi.nlm.nih.gov/29361246/
7 – InformedHealth.org [Internet]. Cologne, Germany: Institute for Quality and Efficiency in Health Care (IQWiG); 2006-. Localized prostate cancer: Learn More – Low-risk prostate cancer: Active surveillance or treatment? [Updated 2022 Sep 16]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK487255/
8 – Kasivisvanathan V, Emberton M, Ahmed HU. Focal therapy for prostate cancer: rationale and treatment opportunities. Clin Oncol (R Coll Radiol). 2013 Aug;25(8):461-73. doi: 10.1016/j.clon.2013.05.002. Epub 2013 Jun 4. PMID: 23759249; PMCID: PMC4042323. https://pmc.ncbi.nlm.nih.gov/articles/PMC4042323/