
 English
English German
German Spanish
Spanish Italian
Italian Japanese
Japanese United states
United states
Prostate cancer care is increasingly centered on a key clinical tension: improving oncologic control while minimizing treatment-related morbidity. In that context, focal laser ablation (FLA) for prostate cancer has emerged as a tissue-sparing approach designed to target a defined intraprostatic lesion rather than treat the entire gland¹. This places FLA within the broader landscape of focal therapy for localized prostate cancer, alongside other energy modalities and image-guided strategies.
For urologists, interest in FLA is typically driven by practical questions: Which patients are appropriate candidates? How should MRI-targeted biopsy and lesion localization guide treatment planning? What do current outcomes suggest regarding in-field control, retreatment, and functional preservation?
This article provides a practical review of MRI-guided focal laser ablation, including patient selection, treatment workflow, and where FLA fits relative to active surveillance, radical prostatectomy, radiation therapy, and other focal therapy modalities in contemporary urologic practice².
What Is Focal Laser Ablation (FLA)?
Above: Illustration of normal prostate gland vs. prostate with cancerous lesions.
Focal laser ablation (FLA) is a form of focal therapy for localized prostate cancer that aims to destroy a defined cancer focus while preserving uninvolved prostate tissue. Instead of treating the whole gland, FLA is lesion-directed and typically integrated into an MRI-based targeting pathway (often built on multiparametric MRI plus targeted biopsy confirmation)³.
Mechanistically, FLA uses laser energy delivered through a fiber placed into the target lesion (via transperineal or transrectal approach, depending on platform/workflow). The laser converts energy to heat, creating thermal coagulative necrosis within the intended treatment zone⁴.
In practical terms, treatment planning focuses on accurate lesion localization, margin design, and protection of nearby critical structures (e.g., urethra, sphincter, neurovascular bundle region), because focal therapy success depends as much on targeting precision as on the energy source itself.
Candidate Selection for Focal Laser Ablation

Selecting patients for focal laser ablation (FLA) should be approached as a structured clinical pathway, not a one-variable decision. Across consensus and guideline-informed discussions, the core principle is to identify men with clinically localized disease in whom a clearly defined target can be treated while preserving function, with full acknowledgment that long-term comparative evidence versus whole-gland therapy remains maturing⁵.
Disease and Lesion Characteristics
The strongest candidates generally have a discrete, MRI-visible index lesion that can be confidently localized and safely treated with an ablative margin.
Contemporary expert reviews emphasize that candidate workup should include multiparametric MRI (mpMRI) plus combined MRI-targeted and systematic biopsy, because disease extent and multifocality assessment are central to deciding whether focal treatment is oncologically reasonable⁶.
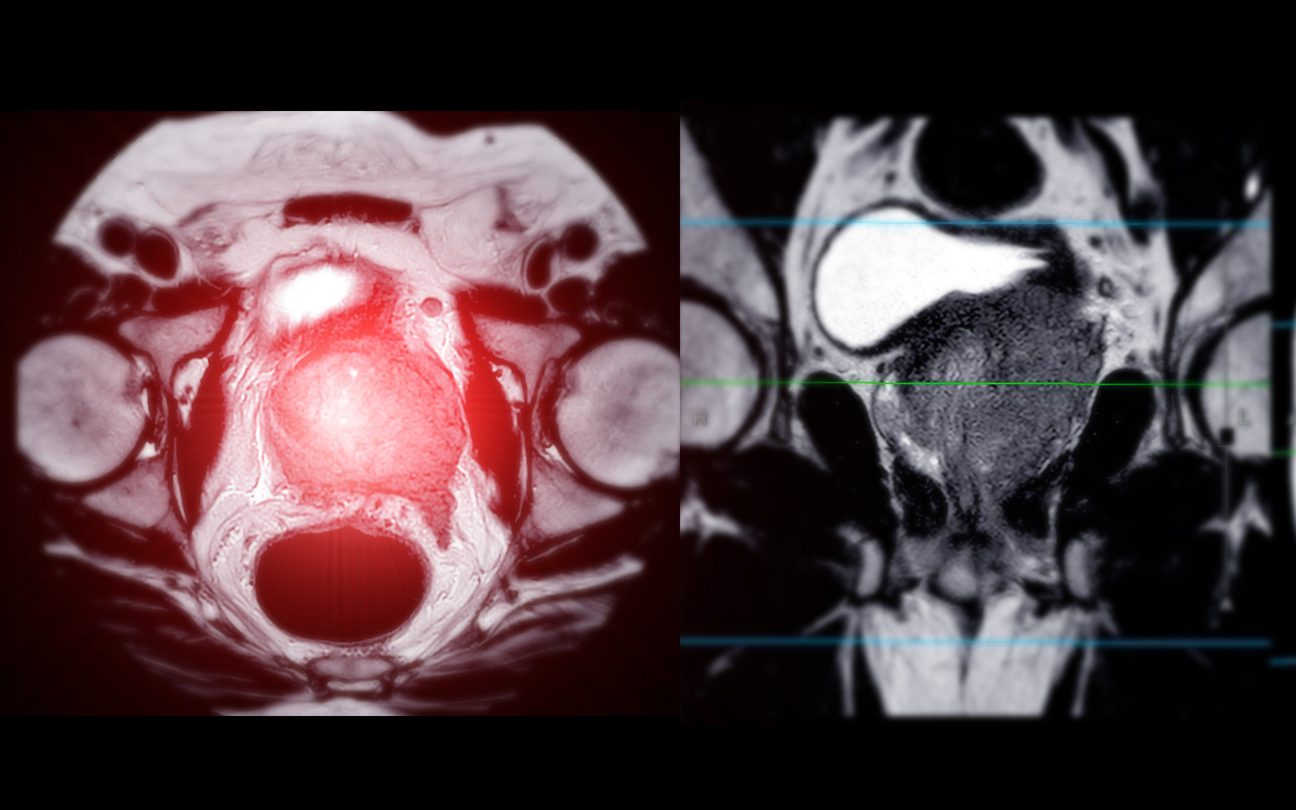
Above: MRI of the prostate gland reveals a focal abnormal signal intensity (SI) lesion at the left posterolateral peripheral zones at the apex.
Clinical Factors
Beyond tumor biology, candidate quality depends on patient-level clinical context: life expectancy, baseline urinary/sexual function, comorbidity profile, and treatment goals (cancer control vs functional preservation).
Consensus-based literature and major guidelines stress shared decision-making so patients understand that focal therapy may reduce whole-gland morbidity exposure but requires disciplined follow-up and carries potential retreatment risk⁷.
Caution Scenarios
Caution is warranted when there is a high likelihood of undertreating biologically or anatomically extensive disease—for example, broad multifocal burden, imaging-pathology discordance, non-localized disease, or lesions that cannot be reliably targeted with acceptable safety margins. In these settings, whole-gland options (or other standard pathways) may be more appropriate⁸.
Procedural Workflow in Practice

In day-to-day urology practice, focal laser ablation (FLA) is best executed as an image-led, protocolized procedure rather than a one-off technical event. A typical workflow starts with pre-procedure confirmation of the index lesion using mpMRI plus histologic confirmation (usually MRI-targeted biopsy with systematic sampling to assess additional disease), followed by treatment planning that defines target geometry and an intended safety margin⁹.
From a practical standpoint, the highest-value technical priorities are: accurate registration/localization, margin-aware ablation planning, and protection of adjacent structures (e.g. urethral and neurovascular regions) to preserve functional outcomes while maintaining oncologic intent.
Key Takeaways for Urologists

For urologists evaluating where focal laser ablation fits in contemporary prostate cancer care, the practical question is not simply whether the technology works—it is whether it can be deployed safely, reproducibly, and within a disciplined longitudinal pathway.
These key takeaways summarize the clinical and operational principles that matter most: selecting the right patient, executing precise image-guided treatment, and maintaining rigorous post-ablation surveillance to protect oncologic outcomes over time.
• Focal laser ablation (FLA) is best viewed as a lesion-directed strategy within a structured focal-therapy pathway, not a replacement for all definitive whole-gland treatments. Current guidance supports cautious adoption with clear patient counseling on evidentiary maturity.
• Patient selection is the main determinant of quality outcomes. Strong candidates generally have localized disease with a clearly targetable, MRI-visible index lesion and imaging-pathology concordance from MRI-targeted systematic biopsy.
• Procedure quality depends on precision steps: reliable target localization/registration, margin-aware ablation planning, and protection of adjacent critical structures to balance oncologic intent with functional preservation.
Finally, set expectations early that surveillance is mandatory. Post-ablation management should combine PSA kinetics, interval mpMRI, and selective confirmatory biopsy, because recurrence may be in-field or out-of-field and cannot be excluded by one test alone.
Are you looking to start a focal therapy program? Contact us to learn more about KOELIS Trinity® and if adding a 3D MRI fusion platform is right for you.
References
1 – Lasorsa, F., Biasatti, A., Orsini, A., Bignante, G., Farah, G. M., Pandolfo, S. D., Lambertini, L., Reddy, D., Damiano, R., Ditonno, P., Lucarelli, G., Autorino, R., & Vourganti, S. (2025). Focal Therapy for Prostate Cancer: Recent Advances and Insights. Current Oncology, 32(1), 15. https://doi.org/10.3390/curroncol32010015
2 – Javier-DesLoges, J., Dall’Era, M.A., Brisbane, W. et al. The state of focal therapy in the treatment of prostate cancer: the university of California collaborative (UC-Squared) consensus statement. Prostate Cancer Prostatic Dis 27, 579–581 (2024). https://doi.org/10.1038/s41391-023-00702-1
3 – Alabousi, M., et al. (2023) MRI-guided Minimally Invasive Focal Therapies for Prostate Cancer. Radiology, 2023. https://doi.org/10.1148/radiol.230431
4 – Colin P, Mordon S, Nevoux P, Marqa MF, Ouzzane A, Puech P, Bozzini G, Leroux B, Villers A, Betrouni N. Focal laser ablation of prostate cancer: definition, needs, and future. Adv Urol. 2012;2012:589160. doi: 10.1155/2012/589160. Epub 2012 May 16. PMID: 22666240; PMCID: PMC3362007.
5 – Ghoreifi, A., Gomella, L., Hu, J.C. et al. Identifying the best candidate for focal therapy: a comprehensive review. Prostate Cancer Prostatic Dis 28, 684–692 (2025). https://doi.org/10.1038/s41391-024-00907-y
6 – Jost von Hardenberg, et al. Potential Candidates for Focal Therapy in Prostate Cancer in the Era of Magnetic Resonance Imaging–targeted Biopsy: A Large Multicenter Cohort Study, European Urology Focus, Volume 7, Issue 5, 2021, Pages 1002-1010, ISSN 2405-4569, https://doi.org/10.1016/j.euf.2020.09.015.
7 – Ong S, Chen K, Grummet J, Yaxley J, Scheltema MJ, Stricker P, Tay KJ, Lawrentschuk N. Guidelines of guidelines: focal therapy for prostate cancer, is it time for consensus? BJU Int. 2023 Jan;131(1):20-31. doi: 10.1111/bju.15883. Epub 2022 Sep 27. PMID: 36083229; PMCID: PMC10087270.
8 – Wysock JS, Lepor H. Optimizing patient selection for focal therapy-mapping and ablating the index lesion. Transl Androl Urol. 2018 Sep;7(Suppl 4):S519-S525. doi: 10.21037/tau.2018.03.16. PMID: 30363486; PMCID: PMC6178318.
9 – Tay, K. J., Scheltema, M. J., Ahmed, H. U., Barret, E., Coleman, J. A., Dominguez-Escrig, J., Ghai, S., Huang, J., Jones, J. S., Klotz, L. H., Robertson, C. N., Sanchez-Salas, R., Scionti, S., Sivaraman, A., De La Rosette, J., & Polascik, T. J. (2017). Patient selection for prostate focal therapy in the era of active surveillance: An International Delphi Consensus Project. Prostate Cancer and Prostatic Diseases, 20(3), 294-299. https://doi.org/10.1038/pcan.2017.8